Understanding Kuru: The Prion Disease That Transformed Neuroscience
Imagine a disease so baffling, so uniquely tied to a culture's most sacred rituals, that its discovery fundamentally reshaped our understanding of biology itself. This is the story of
Kuru disease, a fatal neurodegenerative disorder that, for decades, silently ravaged the Fore people of Papua New Guinea. Far from being a mere medical curiosity, Kuru's unraveling became a pivotal chapter in neuroscience, providing the first concrete evidence of a revolutionary concept: that misfolded proteins, without any genetic material, could be infectious pathogens. Kuru stands as a stark reminder of the intricate interplay between culture, environment, and genetics, and its profound legacy continues to inform our battle against other devastating neurological conditions today.
What is Kuru? The Prion Paradox Explained
At its core,
Kuru disease is classified as a transmissible spongiform encephalopathy (TSE), a family of rare, fatal brain disorders characterized by distinct sponge-like holes (vacuoles) in affected brain tissue. What sets TSEs, and Kuru specifically, apart from conventional infectious diseases is the culprit: not a virus, bacterium, or parasite, but an infectious misfolded protein known as a prion (PrPSc).
These abnormal prions act like insidious templates, converting normal, healthy prion proteins (PrPC) in the brain into their own misfolded, destructive form. This insidious transformation leads to an unstoppable cascade, where these rogue proteins clump together, accumulate, and gradually destroy brain cells. This process results in progressive neurodegeneration without an inflammatory response, a key characteristic that initially baffled researchers, as inflammation is typically the body's natural defense against pathogens.
Early in its presentation, Kuru earned the poignant moniker "the laughing sickness" or "laughing death" due to the emotional lability and episodes of uncontrollable, involuntary laughter that could manifest in its victims. This seemingly bizarre symptom underscored the profound and widespread neurological damage occurring within the brain, particularly affecting areas responsible for motor control and emotional regulation.
The Tragic History: Kuru Among the Fore People
The tragic narrative of
Kuru disease is inextricably linked to the Fore people, an indigenous group inhabiting the remote Eastern Highlands of Papua New Guinea. For generations, Kuru was an endemic scourge within these communities, casting a long shadow over their lives. The disease’s primary mode of transmission, a practice that shocked the outside world, was ritualistic endocannibalism.
As part of deeply ingrained funeral rites, community members would consume the tissues of deceased relatives, including the brain, believing it to be an act of respect, a way to help the spirit of the deceased pass on, and a means to retain the deceased's 'life force' within the community. This practice, particularly the handling and consumption of highly infectious brain tissue, proved to be a tragically efficient pathway for the infectious prions. Epidemiological studies revealed that Kuru disproportionately impacted women and children, often at a ratio of 2:1 or 3:1 compared to men. This disparity was attributed to their primary role in preparing and consuming the deceased, including the brain – the most infectious part – which men typically avoided.
It was in the 1950s that the scientific world first truly confronted Kuru, thanks to the pioneering work of American physician-scientist D. Carleton Gajdusek and Australian medical officer Vincent Zigas. Their meticulous observations and investigations in the field were instrumental in documenting the disease's unique clinical presentation and its devastating prevalence. The scientific breakthrough came in 1965 when Gajdusek and his team successfully transmitted Kuru to chimpanzees through inoculation with brain material from Kuru victims. This seminal experiment provided irrefutable proof of Kuru's infectious nature, establishing it as the first recognized human prion disease and earning Gajdusek a Nobel Prize in Physiology or Medicine in 1976. This tragic cultural practice and its devastating health consequences are explored in more detail in our article:
Kuru Disease: How Ritual Cannibalism Fueled a Deadly Prion Epidemic.
Symptoms and Progression: A Descent into Neurological Impairment
The clinical course of
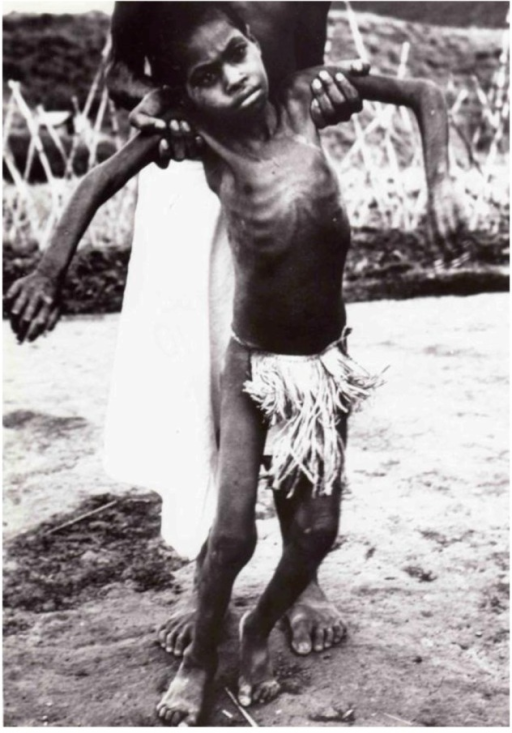
Kuru disease is a relentless and heartbreaking progression through distinct neurological stages, typically leading to death within 3 to 23 months of symptom onset. The disease is characterized by a gradual loss of control over bodily functions, mirroring the relentless destruction of brain tissue, particularly the cerebellum, which is crucial for coordination.
The Ambulant Phase: Early Signs of Distress
This initial stage is marked by subtle yet noticeable signs of neurological dysfunction. Victims often experience an unsteady gait (ataxia), tremors, particularly of the trunk and limbs, and dysarthria (slurred speech). Emotional lability, including the characteristic episodes of uncontrollable laughter, may also begin to manifest. Individuals can still walk, though with increasing difficulty.
The Sedentary Phase: Loss of Independence
As the disease progresses, ataxia becomes severe, rendering the individual unable to walk without support. Tremors intensify, and speech becomes markedly more unintelligible. Dysphagia (difficulty swallowing) develops, posing a serious risk of malnutrition and aspiration. Emotional lability often becomes more pronounced, solidifying Kuru's reputation as the "laughing disease."
The Terminal Phase: Complete Helplessness
In the final, terminal stage, the patient becomes completely immobile, unable to sit up or move voluntarily. They lose control over bladder and bowel functions, becoming incontinent. Swallowing becomes extremely difficult or impossible, often requiring feeding tubes. The individual becomes largely unresponsive to their surroundings, eventually lapsing into a coma before succumbing, frequently to pneumonia or severe malnutrition.
Neuropathologically, Kuru's impact is profound. Autopsies reveal significant cerebellar atrophy, widespread neuronal loss throughout the brain, an increase in glial cells (gliosis), and characteristic amyloid plaques composed of prion protein. The oral route of exposure to the infectious agent likely explains the distinctive predominance of cerebellar involvement, which underpins the severe motor symptoms.
Kuru's Enduring Legacy: Impact on Prion Science and Beyond
The decline of the Kuru epidemic stands as a testament to the power of public health intervention and understanding the root cause of disease transmission. Following concerted efforts by missionaries and governmental bodies in the late 1950s, the practice of endocannibalism among the Fore people largely ceased. This cultural shift led to a sharp and sustained decline in new
Kuru disease cases, to the point where active transmission is now considered extinct.
However, Kuru presented scientists with another astounding revelation: its extraordinarily long incubation periods. While some individuals succumbed within a decade, others developed symptoms more than 50 years after their last potential exposure, with the last known death occurring as late as 2009. These prolonged incubation times underscored the silent, insidious nature of prion diseases and the unique challenges they pose for surveillance and medical understanding.
The study of Kuru profoundly influenced prion research, providing irrefutable evidence for the "protein-only" infectivity hypothesis – a concept initially met with strong skepticism because it challenged fundamental tenets of molecular biology that centered on genetic material (DNA or RNA) for transmission. This paradigm shift was critical for understanding other prion diseases like Creutzfeldt-Jakob disease (CJD) and bovine spongiform encephalopathy (BSE), commonly known as "mad cow disease." While Kuru prions exhibit transmission properties equivalent to those of sporadic CJD, including similar misfolded prion protein (PrPSc) glycoforms and attack rates in animal models, their distinct origin and epidemiological pattern highlight the diverse pathways through which these devastating proteins can emerge and spread.
Furthermore, genetic factors were found to play a crucial role in susceptibility to Kuru. Polymorphisms at codon 129 of the
PRNP gene, which codes for the prion protein, significantly modulated risk, with methionine homozygotes being at higher risk. Intriguingly, a novel variant (G127V) was discovered that conferred strong protection against Kuru, suggesting a rapid evolutionary adaptation within the Fore population against prion diseases. The mysteries surrounding Kuru's unique epidemiology and its scientific breakthroughs are further explored in
Kuru Explained: From "Laughing Death" to Extinct Prion Mystery.
Kuru's legacy extends beyond its direct epidemiology. Its study informed our understanding of the risks of iatrogenic transmission – the accidental spread of disease through medical procedures, such as via contaminated surgical instruments or tissue grafts, as prions are notoriously resistant to conventional sterilization methods. More broadly, Kuru provided a foundational model for understanding protein misfolding as a pathogenic mechanism, a concept now central to research into other widespread neurodegenerative conditions like Alzheimer's, Parkinson's, and Huntington's diseases. The lessons learned from Kuru continue to guide ongoing research into these devastating illnesses, highlighting the critical role of protein structure and dynamics in brain health and disease.
Conclusion
From the remote highlands of Papua New Guinea,
Kuru disease emerged not just as a devastating local epidemic, but as a global scientific enigma that forever altered our understanding of infectious agents and neurodegenerative processes. Its unique etiology, inextricably linked to a specific cultural practice, provided a tragic yet invaluable natural experiment. The painstaking work of Gajdusek and others transformed Kuru from a perplexing "laughing death" into a cornerstone of modern prion science, proving the revolutionary concept of protein-only infectivity. While Kuru transmission has ceased, its echoes resonate in every laboratory studying protein misfolding and in every medical guideline addressing iatrogenic risk. Kuru stands as a powerful reminder of the intricate interplay between culture, genetics, and environment, and its study continues to illuminate pathways to combating some of humanity's most challenging neurological diseases.